Is It Too Late? How Age Really Affects Your Fertility

Is it too late?
That's the question underneath every search about age and fertility. You've read the statistics and seen the charts that make 35 look like a cliff. They tell you what happens on average. They don't tell you whether it's too late for you.
Here's the direct answer: for most women asking this question, it is not too late. But what "not too late" looks like depends on your specific situation, not your age bracket. The next step is understanding what's actually changing in your body, what makes your picture unique, and how to get your own answer.
What's Changing in Your Body (and What Isn't a Cliff)
A lot of the fear around age and fertility comes from not knowing what's actually happening versus what the internet makes it sound like. It's true that fertility decreases with age. But that's the starting point, not the whole story. Here's the biology in concrete terms.
Egg Supply, Egg Quality, and What the Numbers Look Like
Your egg supply goes down over time. You're born with roughly 1 to 2 million eggs, have about 300,000 to 500,000 by puberty, and lose them faster starting in the mid-to-late 30s. Egg quality changes too. As you get older, more of your eggs have the wrong number of chromosomes. By around 40, most of them do. That makes it harder to conceive and raises the risk of miscarriage. But this is a gradient, not a cliff. Younger women produce eggs with chromosome issues too. It's just that the ratio changes over time, not all at once.
One common question: does hormonal birth control affect your egg reserve? It doesn't. Ovulation is suppressed while you're on it, but the underlying process of follicle loss continues at the same pace. Being on birth control for years doesn't save eggs or use them up faster.
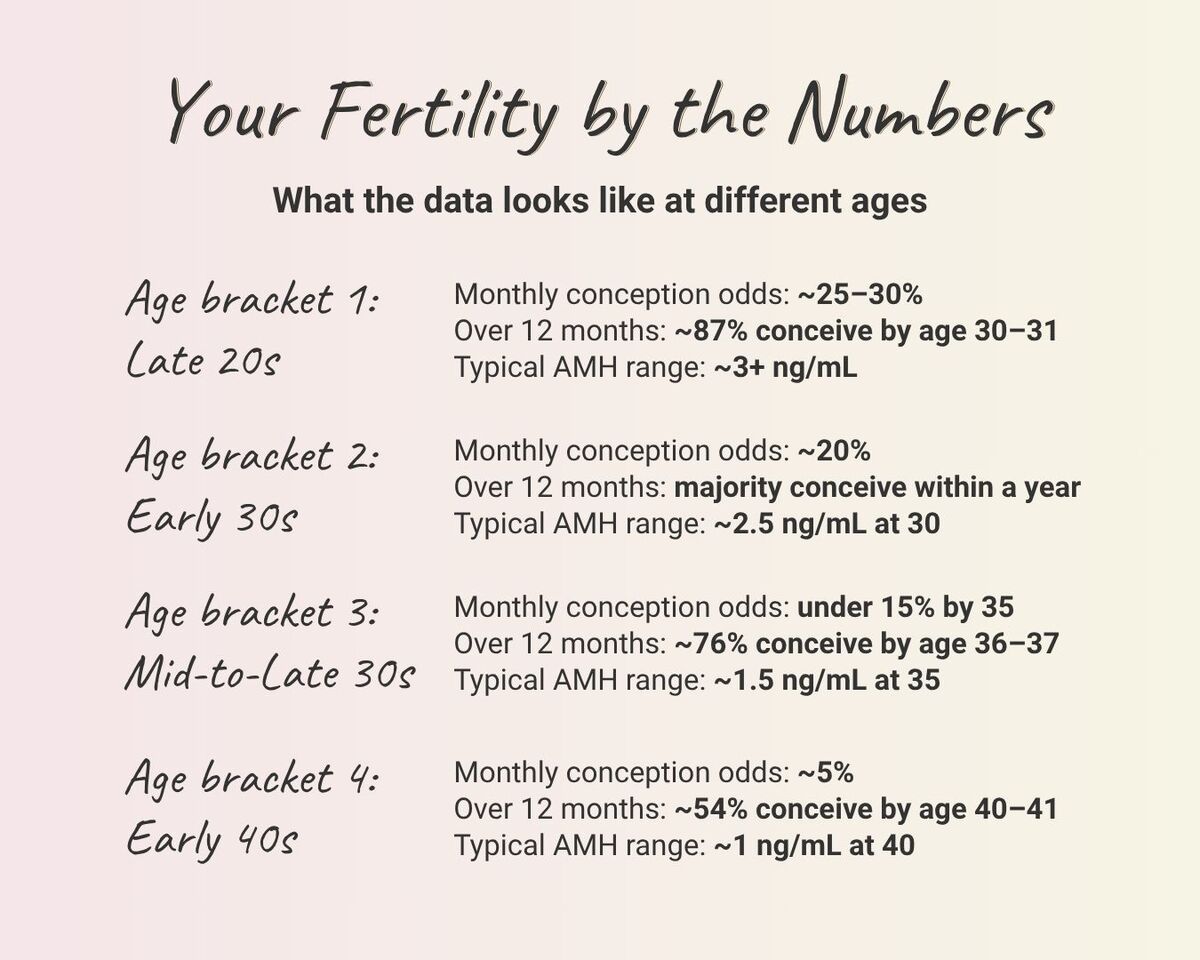
The per-cycle odds can feel alarming: about 25 to 30% in the early-to-mid 20s, roughly 20% at 30, under 15% at 35, around 5% at 40. But per-cycle isn't the full picture. Over 12 months, the majority of women in their early 30s conceive, and more than half of women at 40 do too.
What You Can't See (and How Testing Can)
The changes happening in your eggs and ovarian tissue don't always show up in ways you'd notice. Sometimes cycles get shorter or less regular over time, but many women don't see any obvious signs at all. Your anti-Müllerian hormone (AMH) and follicle-stimulating hormone (FSH) levels are shifting whether or not your cycle looks different. That's why testing matters. It picks up what you can't see on your own, and tracking those patterns gives your provider a much clearer picture than your age or your cycle alone.
Recent research from UCSF has shown that age-related changes go even deeper. The ovarian tissue surrounding your eggs, including supporting cells, nerves, and connective tissue, changes with age, too. That's part of why two women the same age can have very different fertility outlooks, and why individual testing matters more than averages.
Your Age Isn't Your Whole Answer
Biology sets a baseline. But your individual fertility picture has more inputs than your birthday.
Two people the same age can have meaningfully different outlooks. Your diagnosis, your medical history, and your partner's health all shape what that curve looks like for you.
Women with PCOS, for example, often maintain higher ovarian reserve into their late 30s. In large IVF cohorts, PCOS patients had higher pregnancy and live birth rates than age-matched patients with tubal factor up to about age 40. After 40, those outcomes converged. Age does become the dominant factor eventually. But before that point, PCOS changes the math in ways that population averages don't reflect.
Endometriosis can push in the opposite direction. It sometimes accelerates ovarian aging regardless of chronological age. A 32-year-old with endometriosis may face a reserve profile that looks more like 37.
Male partner age matters too. Sperm quality declines gradually. Measurable effects on conception time and IVF outcomes start to show around 40. This applies regardless of the female partner's age.
The point isn't to catalogue every variable. It's that your answer to "is it too late" depends on more than your birthday. The way to find out which factors apply to you is to look.
How to Get Your Actual Answer
So far, everything in this blog has been about patterns and populations. The question you came here with is personal. Testing is how you make it personal.
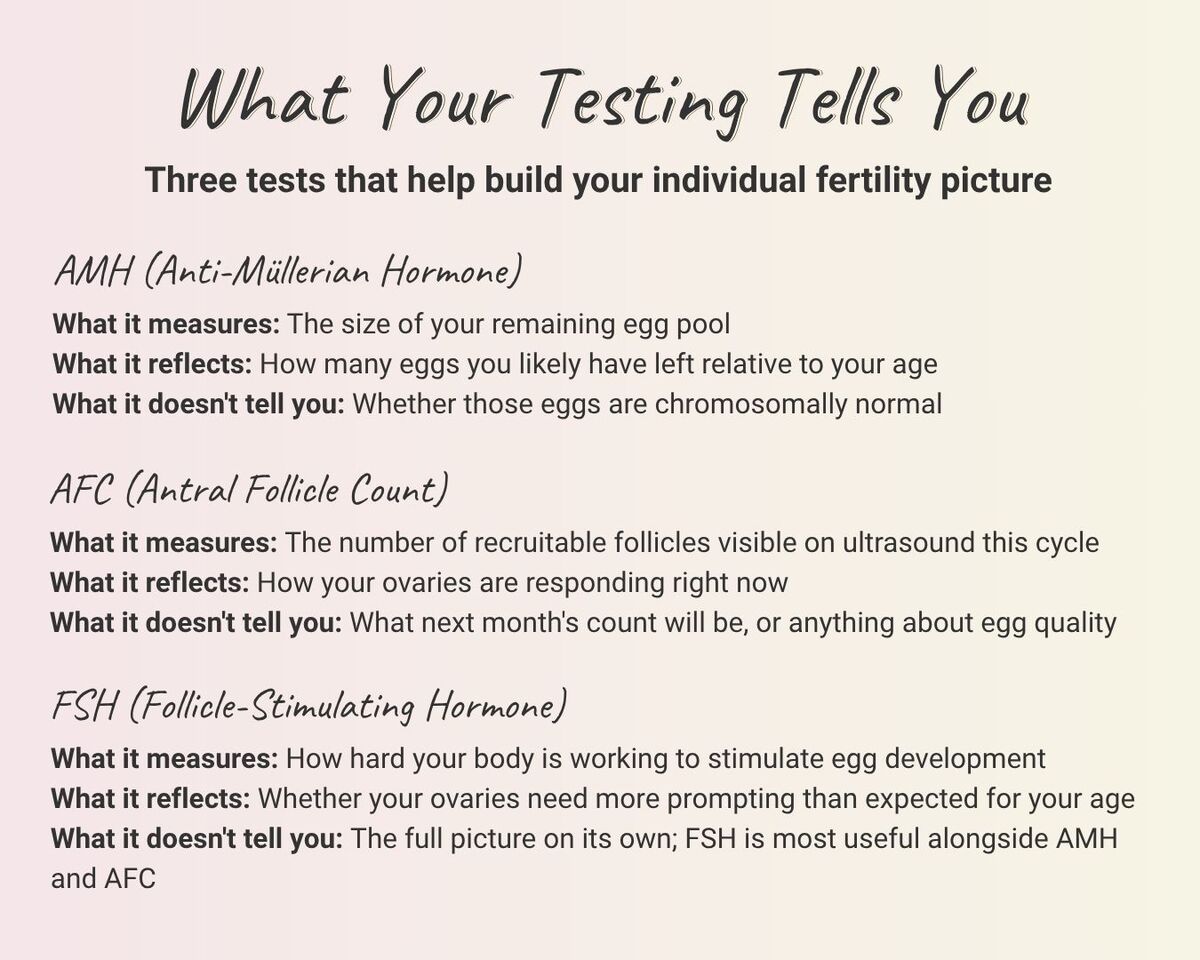
These three tests form the core of an individual fertility picture. They give your provider information that your age alone can't. One limitation worth naming: none of them measure egg quality. AMH, AFC, and FSH assess quantity and ovarian function. Chromosomal normality is where preimplantation genetic testing enters. That happens during treatment, not initial evaluation.
Age tells you where the population average sits. Testing tells you where you sit. Some 34-year-olds have diminished reserve. Some 39-year-olds have stronger numbers than their age would predict. The gap between the average and the individual is often wider than people expect, in both directions. The only way to know is to look.
What "Not Too Late" Looks Like from Here
Knowing where you stand changes the conversation. Once you have your own data, the path forward starts to take shape. Your results, your history, and your goals all factor into what comes next.
For many patients with good reserve and no severe complicating factors, IUI is a strong starting point. When reserve, quality, or other factors shift the calculus, IVF becomes a more likely path. And fertility preservation is worth discussing early, not only when time feels short. Freezing eggs or embryos at a younger age preserves quality at the time of freezing, which gives you more flexibility later.
The reason recommendations shift isn't that one option is better than another. It's that each one fits a different clinical picture. What matters is that yours is based on your results, not on a generalized chart you found online.
"Not too late" almost always means there's a plan. The specifics of that plan are what a consultation is for.
Take the Next Step at The Fertility Wellness Institute of Ohio
The only version of "too late" that actually matters is the one where you never find out where you stand. Everything else is a conversation with real data, real options, and a path forward.
At The Fertility Wellness Institute of Ohio, that conversation starts with your individual testing and a transparent look at what the results mean for you. Your age is one input. Your full picture is what shapes the plan.
If you've been carrying the question, bring it. Contact us to schedule a consultation where your data, not a population average, drives the answer.